
“It’s All In Your Head” - the long history of dismissing women’s health
The word hysterical gets thrown around casually to describe an overreacting person, an out-of-control crowd, or a comedian who had the audience loudly cackling. Most people have no idea that the word carries more than 4,000 years of medical history in its etymology. And that history is not funny at all.
It is a history of women being dismissed, institutionalized, misdiagnosed, and mistreated - not because medicine didn't care about getting it right, but because medicine was built on a foundation that assumed women's bodies and minds were fundamentally unreliable. Understanding where that assumption came from, and how it persists today, is essential for anyone who wants to understand why women are still fighting to be believed in the exam room.
The Word Itself: Hysteria and the “Wandering Womb”
The oldest record of hysteria dates back to 1900 BCE, when Egyptians recorded behavioral abnormalities in adult women on the Kahun Papyrus, attributing the disturbances to a wandering uterus, but it was not called hysteria back then in Ancient Egypt.
The word hysteria derives from the ancient Greek hystera, meaning uterus. The Greek notion was that hysteria was peculiar to women and caused by disturbances of the uterus - in fact floating around in the abdomen and “bumping” into organs causing disease and dysfunction. The womb was imagined as a kind of rogue organ (lol) - moving upward to compress the heart or throat, or drifting sideways toward the liver or spleen. The 2nd-century physician Aretaeus described the uterus as "a female viscus, closely resembling an animal," wandering every which way throughout the body.
This theory was repeated by Hippocrates, Plato, and Celsus. It would remain remarkably influential for the next two thousand years, and unfortunately this notion is still prevalent today.
Ancient Egypt and Greece: 1900 BCE – 5th Century BCE
Plato's Timaeus included an account of something akin to hysteria - a condition in which the womb, remaining barren beyond its natural time, becomes distressed and wanders throughout the body, obstructing passages and causing suffocation and various diseases. The prescribed cure was predictable: marriage and pregnancy, which would give the uterus its proper purpose and keep it in place. Does this sound familiar to how sometimes physicians will tell patients that pregnancy will cure period problems or things such as endometriosis?
Ancient Roman physicians discarded the literal wandering womb theory but retained the fundamental premise. They credited hysteria to a disease of the womb or a disruption in reproduction- such as a miscarriage or menopause (oh and so this is where miscarriage and menopause became taboo!). The organ was still to blame. The woman was still defined by her reproductive capacity, or the lack of it. This is why you will hear me say - women’s health has been and still does become boiled down to her reproductive potential.
What's notable about this era is that the symptoms attributed to hysteria were real. Seizures, paralysis, difficulty breathing, emotional distress, fainting - these were genuine experiences that even the outsider could see. What was wrong was not the observation but the explanation, and more crucially, the solution: not treatment, but correction of the woman's failure to fulfill her reproductive role.
The Middle Ages: Witchcraft, Demons, and Punishment
If ancient medicine pathologized the uterus, the medieval period added a theological layer that made things considerably more dangerous. During the Renaissance period, many patients of what would have been labeled hysteria were prosecuted as witches and underwent interrogations, torture, exorcisms, and execution.
Throughout history, medical treatments for these "female problems" ranged from hanging women upside down and shaking them to return the uterus to its rightful place, to putting leeches in the vagina, to giving suppositories of bull urine. These were not fringe practices - they were mainstream medicine.
The 17th and 18th Centuries: Medicalization and the "Mother"
By the early 1600s, the language of hysteria was shifting from the purely supernatural to medical. Long before "hysteria" entered English, the name for this supposed condition was "suffocation of the mother" - the "mother" being a colloquial term for the womb.
Early medical texts of this era described the condition in physical terms - a rising, a suffocation, a fit - that roughly corresponded to what we would now recognize as panic disorder or conversion disorder. The treatments remained a mix of the bizarre and the harmful: purges, fumigation, bloodletting, and herbal remedies. Cool.
Trota de Ruggiero, considered the first female physician in Christian Europe and the first gynecologist, recognized that women were often ashamed to go to a doctor with gynecological issues (the still are, Dr. Trota). She studied women's diseases and prescribed remedies such as mint for women suffering from hysteria. Her work was unusual for acknowledging that women's suffering deserved serious clinical attention - a perspective that some would argue is still rare today.
The 19th Century: The Victorian Era and the Height of Hysteria
The Victorian period represents the apex of hysteria as a cultural and medical phenomenon. Hysteria was the most well-known and frequently recorded mental illness of women during the Victorian period - a diagnosis often given by default, when doctors couldn't come up with any other explanation.
In 1859, one physician claimed that over a quarter of all women suffered from hysteria. The possible symptoms list was staggering. One American physician, George Beard, compiled what amounted to a catalog of nearly every symptom a human being can experience and labeled them all potential signs of hysteria in women. Is it suffice it to say this was the first list of perimenopausal symptoms?! Maybe he was on to something - HAH.
A woman could be considered "unbalanced" due to causes including menstruation-related anger, pregnancy-related sadness, postpartum depression symptoms, disobedience, chronic fatigue, anxiety, and even daring to ask for a divorce. The asylum was not only a medical institution in the Victorian era; it was a mechanism of social control.
The "rest cure," popularized by Dr. Silas Weir Mitchell, involved strict bed rest, isolation from family and friends, a high-calorie diet, and minimal mental stimulation. This treatment was intended to calm the nervous system but often leading to further mental distress and helplessness. The writer Charlotte Perkins Gilman famously documented the psychological devastation of this "treatment" in her 1892 short story The Yellow Wallpaper, one of the most precise literary accounts of medical cruelty dressed up as care.
Meanwhile, in Paris, neurologist Jean-Martin Charcot was staging something rather different. At the Pitié-Salpêtrière, Charcot staged weekly "hysteria shows," transforming medical lectures into theatrical events in which female patients became the main attraction. During the 1870s and 1880s, crowds of students, visiting physicians, and curious members of high society gathered as Charcot hypnotized patients and guided them into dramatic poses such as arching backs, rigid limbs, in what were billed as scientific demonstrations.
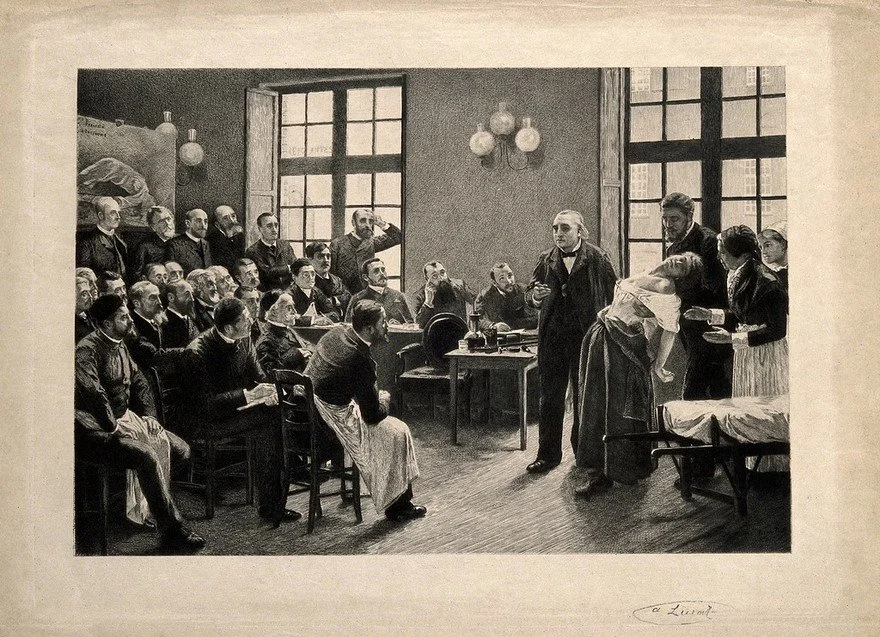
Charcot's work did, in some ways, move the field forward. He argued that hysteria derived from a neurological disorder rather than the supernatural, dispelling beliefs that it had anything to do with witchcraft, and attempted to define it medically. He also argued that hysteria was more common in men than women (can I get an amen). But the women in his demonstrations were still spectacles, still objects of study rather than patients deserving care.
His student Sigmund Freud took the work further still. Freud researched the psychological aspects of hysteria and coined the term hysterical conversion, which referred to how unpleasant memories (trauma) could manifest as physical symptoms. His recognition of trauma's role was genuinely significant. But Freud also tied hysteria deeply to female sexuality and to what he framed as women's inherent psychological deficits. This was groundwork that would shape how women's mental and physical symptoms were interpreted for much of the 20th century. Reminder: you are not broken. Our today’s problem is a result of centuries of influential leaders shaping how we view womanhood even today.
The 20th Century: A New Name, the Same Dismissal
The formal diagnosis of hysteria faded across the 20th century as psychiatry advanced, and individual conditions such as epilepsy, conversion disorder, anxiety, depression began to be differentiated and diagnosed more accurately. However it was not until 1980 (!!!!), "hysterical neurosis" was finally officially removed from the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM), replaced by the modern diagnosis of conversion disorder.
But removing the word did not remove the belief system behind it. The assumption that women's symptoms have emotional rather than physical origins, that women exaggerate their pain, that women are fundamentally less reliable narrators of their own bodily experiences did not disappear with the DSM revision. If you want to read more about this, you should check out The Pain Gap by Anushay Hossain.
There are many conditions that disproportionately affect women: autoimmune diseases, anxiety, depression, chronic pain, chronic fatigue. Across the 20th century, they were routinely dismissed as psychosomatic, as "stress," as attention-seeking. Women presenting with these conditions were told to lose weight, referred to a therapist, prescribed benzodiazepines or opioids or told there is nothing really wrong with them. Another book recommendation here is - Unwell Women, Misdiagnosis and Myths in a Man-Made World by Elinor Cleghorn (my all time favorite book and inspiration to this blog post).
Today: The Legacy Is Still Very Much Alive
Considering that the word hysteria was not removed from the DSM until 1980, the sentiment is still alive and well today.
In a national survey of nearly 2,600 women with chronic pain conditions, 65% felt their pain was being given inadequate attention because they were female, 91% believed the healthcare system discriminated against women, nearly half were told their pain was psychological, and 75% were told they must learn to deal with it.
Women are seven times more likely than men to be misdiagnosed and discharged during a heart attack, AND if they are diagnosed with a heart attack, they are more likely to die from it than a man.
In the United States, women wait an average of 65 minutes before receiving an analgesic for acute abdominal pain, while men wait only 49 minutes. Women with acute abdominal pain are up to 25% less likely than men to be treated with opioid painkillers, and middle-aged women with chest pain are twice as likely as men with the same symptoms to be diagnosed with a mental illness.
Women are roughly 20 to 30% more likely than white men to be on the receiving end of a diagnostic error - and for women of color, that risk is even higher (see my blog post:).
Conditions like endometriosis take an average of 7 to 10 years to diagnose, largely because the pain has been normalized or attributed to anxiety. Women with Von Willebrand's disease - a bleeding disorder - face a delay of 16 years between symptom onset and diagnosis, despite being more likely than men to notice the symptoms. The diagnostic gap for autoimmune diseases, which affect women at disproportionately high rates, is well documented.
The Throughline
From the Kahun Papyrus in Egypt to the modern emergency department, the core narrative has been remarkably consistent: women's bodies are mysterious, their symptoms unreliable, their pain excessive, their distress emotional. The name changed - from wandering womb to hysteria to psychosomatic to anxiety - but the effect was the same. Women's legitimate suffering was ignored instead of treated.
Our contemporary biomedical knowledge is stained with the residue of old stories, lies, assumptions, and myths. The historical idea that women's excessive emotions have profound influences on their bodies is impressed like a photographic negative beneath today's image of the attention-seeking, hypochondriac female patient.
Changing this requires more than individual clinicians making better choices, though that matters enormously. It requires overhauling research infrastructure to include women at every stage, from basic science to clinical trials. It requires medical education that teaches the history of gender bias as foundational knowledge, not an elective afterthought. It requires that patients, especially women, be believed as the primary experts on their own experience.
And it requires that all of us, clinicians and patients alike, understand that when a woman says something is wrong, 4,000 years of "it's all in your head" is not a neutral backdrop. It is the context in which she is speaking, and it shapes everything about whether she will be heard.
This article is intended for educational purposes and does not constitute medical advice.